A State Policy Brief from the national JIWC
April 2023
Executive Summary: Only 6 states have laws with written policies on breastfeeding support for incarcerated postpartum people in the U.S. This is a critical gap in public health policy because breastfeeding is vital to infant and postpartum health and well-being.
Background:
Historically, the intersection of pregnancy-related outcomes in carceral contexts has been under-researched.1 As a result, there are limited policies and programs that directly serve the unique needs of incarcerated pregnant and postpartum people. For most incarcerated people, birth is followed by near immediate separation from their newborn: biological mothers return to prison and infants are placed with alternative caregivers in the community.2, 3 Rarely are postpartum people in custody given the resources they need to successfully breastfeed or sustain their milk supply through pumping and milk storage.4
Breastfeeding is an essential component of health for newborns and postpartum people alike; breastfeeding confers a variety of immunological, developmental, and psychological benefits for both mother and child across the lifecourse. Unless otherwise indicated, exclusive breastfeeding for the first six months of life is recommended by a variety of health organizations–including the World Health Organization and American Academy of Pediatrics.5 Even in instances where breastfeeding cannot be sustained for six months, early initiation of breastfeeding (within the first few hours and days after birth) provides newborns with colostrum, which dramatically reduces an infant’s risk of contracting infectious diseases.6
Though limited, there are some state laws that provide specific considerations for individuals who are breastfeeding or support breastfeeding in carceral settings.2 Some state laws facilitate breastfeeding by allowing incarcerated postpartum people to live with their infants in prison nursery programs or community-based settings. In states where separation is routine, some state laws allow postpartum people to pump and store breastmilk, which is then delivered to their newborn who may be living with extended, foster, or adopted families. Other states provide support and education before and after birth.5 This report summarizes state laws related to breastfeeding support for incarcerated pregnant and postpartum people in the U.S.
State Laws:
6 states have laws with written policies on breastfeeding support for incarcerated postpartum people in the U.S.
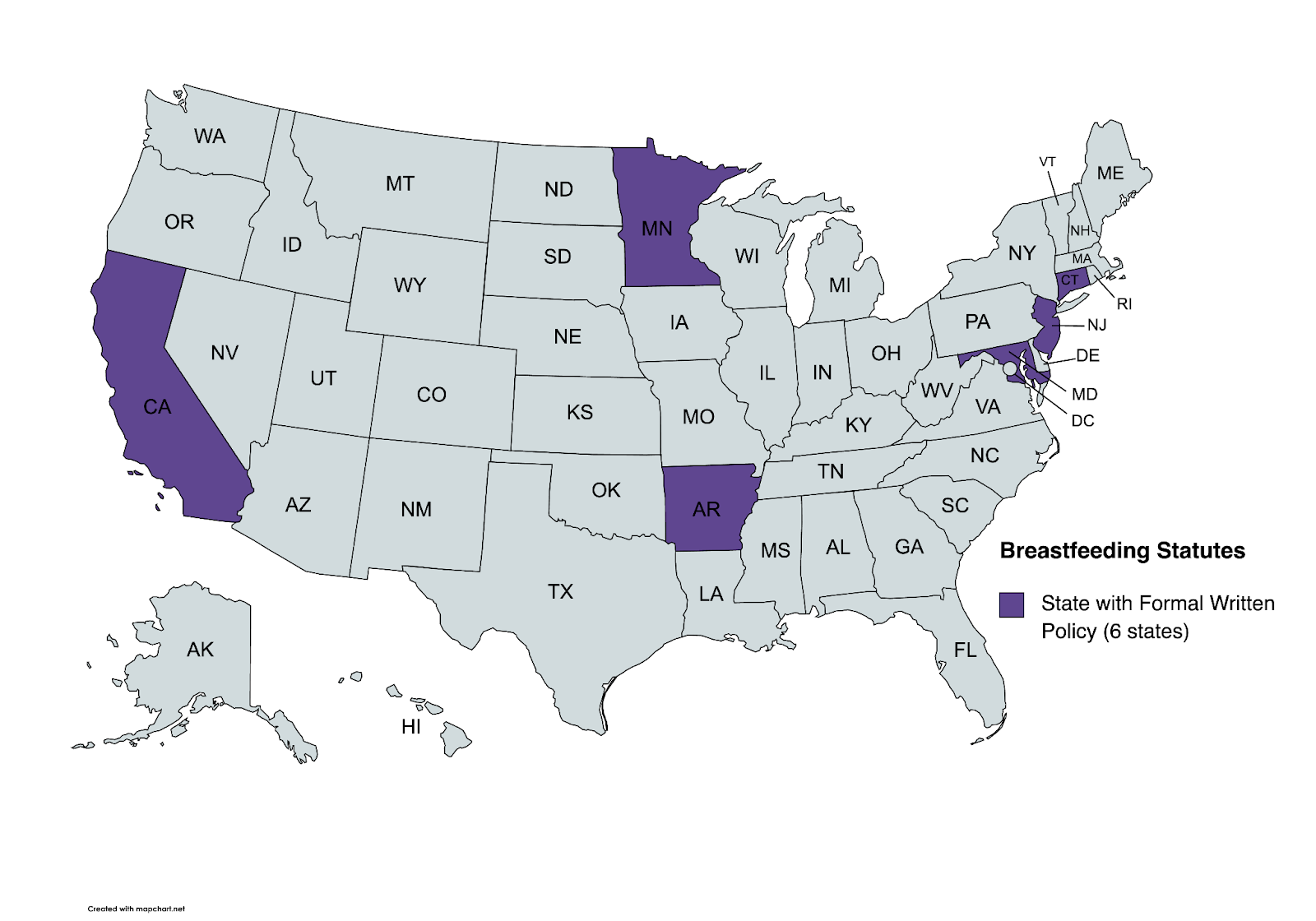
Arkansas prohibits the placement of pregnant people, recently postpartum (within 30 days of birth) individuals, people being treated with postpartum depression, and those currently breastfeeding in restrictive housing (solitary confinement) for 30 or more days unless there is “reasonable cause” to believe they pose a substantial or imminent threat to another person.
Maryland and Connecticut require that incarcerated postpartum people can pump and store breastmilk for delivery to their babies.
Minnesota requires that incarcerated postpartum people receive education and resources to support breastfeeding. Minnesota is one of 12 states that have state laws to prevent the separation of postpartum people from their newborn which can help to facilitate breastfeeding.
California and New York detail more comprehensive breastfeeding policies for incarcerated postpartum people. California requires that sheriffs in county jails develop and implement an “infant and toddler breast milk feeding policy” including procedures for the expression, storage, and delivery of breastmilk to the person’s child. Participation is conditional on drug screening. California also requires that incarcerated pregnant people have access to a social worker who discusses the benefits of lactation, feeding plans, and newborn care.
In New York, postpartum people who are breastfeeding are able to reside with their babies in prison nursery programs until the baby is one year of age, or eighteen months if the person is to be granted parole shortly thereafter. This law is most comprehensive as it keeps newly postpartum people living with their babies making exclusive breastfeeding more feasible.
A comprehensive, sortable table of these summaries (including links to relevant statutes) can be accessed here.
Other states, like Alabama and Arkansas, have robust programming to support incarcerated breastfeeding people, even in the absence of state laws to codify these practices. For example, the Alabama Prison Birth Project worked with Julia Tutwiler Prison for Women to open rooms for incarcerated people to pump, store, and ship milk to their newborns who reside outside of the prison. Similarly, University of Arkansas for Medical Sciences (UAMS) worked with the Arkansas Department of Corrections to open a space for postpartum people to pump milk, and sometimes even breastfeed during visits with their babies as part of a program called Growing Together.
12 states (California, Illinois, Ohio, Maryland, Minnesota, Missouri, New Jersey, New York, Tennessee, Texas, West Virginia, and Wisconsin) have state policies providing alternatives to incarceration for pregnant and postpartum people through alternative sentencing models, prison nursery programs, and community-based alternatives. These policies typically delay or prevent the separation of postpartum people from their babies which may provide solutions/alternatives. To learn more about these alternatives, check out the March 2023 state-by-state policy brief on this topic.
Permissive Prison Policies & Low Rates of Lactation:
There are only six states with state laws related to breastfeeding support for incarcerated people. Only one-third of U.S. prisons and jails have any written policy on breastfeeding.2 According to one study from Asidou, Beal, and Sufrin (2021) even in settings with supportive policies, rates remain exceptionally low.4 The authors concluded: “…structural constraints of unsupportive policies may lead to undesired and coerced weaning and limit health benefits related to the mother–infant dyad.”4 This evidence suggests that low rates of breastfeeding likely persist even in states with supportive laws.
Several barriers exist. First, policies on lactation may not be adequately communicated or enforced amongst prison and jail personnel or healthcare providers.4 Moreover, incarcerated people may not have access to adequate education, postpartum plans, or support to initiate and sustain breastfeeding.4 Additionally, policies may not outline procedures for the proper storage, management, and delivery of getting pumped milk to babies who reside outside of the facility.4 Lastly, stigma (including internalized stigma) may lead people to believe that it is not safe or optimal for incarcerated mothers to breastfeed their babies.
Recommendations:
- Keep Postpartum People with their Infants using Alternatives to Incarceration: To best facilitate opportunities for breastfeeding, infants need to be with their mothers. Therefore, policies and programs should aim to keep postpartum people with their infants following birth either through alternative sentencing, prison nursery programs, or community-based alternatives. Prison policies that support breastfeeding should be codified in state law to reduce the risk that policies are changed when there are changes in prison leaders and administrators.
- Invest in Lactation Support Programs: Even in instances where states do not have state laws, facilities can partner with prison doula programs and lactation support services to fill existing gaps postpartum. Programs that provide education, material support, and space for incarcerated people to pump and store milk for delivery (and/or breastfeed during family visitation hours) can serve as critical intervention in the absence of a state law.
- Develop and Distribute Cross-systems Education: Healthcare providers and personnel working in prisons and jails should be educated on the standard of care for breastfeeding postpartum people who are incarcerated. For example, healthcare providers should support early initiation of breastfeeding even in instances where postpartum people will be separated from their newborns following birth.
Key Conclusions:
Incarcerated people often have inadequate postpartum care, including care and resources for breastfeeding and lactation. Even in states with existing laws, breastfeeding rates in U.S. prisons and jails remain extremely low. Separating postpartum people from their babies following birth impedes bonding and attachment, and is in direct opposition to health recommendations to promote exclusive breastfeeding for the first six months of a baby’s life. Whenever possible, policymakers should pursue alternatives to incarceration so that incarcerated mothers are not separated from their babies. Policies like these can improve family health in a myriad of ways, including by promoting breastfeeding. In cases where this is not possible, postpartum people in custody should have access to lactation rooms where they can pump and store breastmilk for delivery to their newborn. In sum, breastfeeding promotes optimal maternal and infant health, and should be a key feature of postpartum healthcare for incarcerated populations.
Suggested Citation:
Laine, R., Benning, S., & Shlafer, R. (2023). Breastfeeding and Lactation Support for Incarcerated People in the U.S. Center for Leadership Education in Maternal and Child Public Health, University of Minnesota.
Designed by Cassie Mohawk, The Center for Leadership Education in Maternal and Child Public Health (mch@umn.edu).
Acknowledgements:
Funding for this effort was provided by the Center for Leadership Education in Maternal and Child Public Health at the University of Minnesota. The Center is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number T76MC00005-67-00 for Leadership Education in Maternal and Child Public Health in the amount of $1,750,000. This information or content and conclusions of related outreach products are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
References:
- Bronson, J., & Sufrin, C. (2019). Pregnant Women in Prison and Jail Don’t Count: Data Gaps on Maternal Health and Incarceration. Public Health Reports, 134(1_suppl), 57S-62S. https://doi.org/10.1177/0033354918812088
- Wang, L. (2021). Unsupportive environments and limited policies: Pregnancy, postpartum, and birth during incarceration. Unsupportive Environments and Limited Policies: Pregnancy, Postpartum, and Birth during Incarceration.
- Pendleton, V. E., Schmitgen, E. M., Davis, L., & Shlafer, R. J. (2021). Caregiving arrangements and caregiver well-being when infants are born to mothers in prison. Journal of Child and Family Studies, 1-14.
- Asiodu, I. V., Beal, L., & Sufrin, C. (2021). Breastfeeding in Incarcerated Settings in the United States: A National Survey of Frequency and Policies. Breastfeeding Medicine: The Official Journal of the Academy of Breastfeeding Medicine, 16(9), 710–716. https://doi.org/10.1089/bfm.2020.0410
- CDC. (2021, July 27). Five Great Benefits of Breastfeeding. Centers for Disease Control and Prevention. https://www.cdc.gov/nccdphp/dnpao/features/breastfeeding-benefits/index.html
- Kotlar, B., Kornrich, R., Deneen, M., Kenner, C., Theis, L., von Esenwein, S., & Webb-Girard, A. (2015). Meeting Incarcerated Women’s Needs For Pregnancy-Related and Postpartum Services: Challenges and Opportunities. Perspectives on Sexual and Reproductive Health, 47(4), 221–225. https://doi.org/10.1363/47e3315
- Shlafer, R. J., Davis, L., Hindt, L. A., Goshin, L. S., & Gerrity, E. (2018). Intention and Initiation of Breastfeeding Among Women Who Are Incarcerated. Nursing for Women’s Health, 22(1), 64–78. https://doi.org/10.1016/j.nwh.2017.12.004
- Reproductive Health Care for Incarcerated Pregnant, Postpartum, and Nonpregnant Individuals | ACOG. (2021). ACOG: The American College of Obstetricians and Gynecologists Clinical. Retrieved December 12, 2021, from https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2021/07/reproductive-health-care-for-incarcerated-pregnant-postpartum-and-nonpregnant-individuals